- Bladder stones are the most common type of the lower tract calculi
- Migrant bladder stone
- Calculi formed in the upper urinary tract and then migrated in the urinary bladder.
- Primary bladder stone
- Related to vitamin deficiency and low dietary intake of the animal protein and phosphate
- Prevalent in North Africa, Middle and far East
- Commonly develop in children younger than 10 years and more common in boys
- Most common solitary stone
- The stone composition commonly calcium oxalate, uric acid, calcium phosphate
- Secondary bladder stone
- Related to bladder outlet obstruction
- BHP, bladder neck structure, neurogenic bladder: Main cause of bladder calculi
- Stones composed of uric acid, calcium oxalate or triple phosphate
- Related to urinary tract infection
- Urease producing bacteria are responsible
- Stones usually composed of triple phosphate and carbonate apatite
- Related to catheterization
- Patient with urethral or suprapubic catheter have increased risk
- Related to foreign body
- Iatrogenic foreign body (fragments of burst balloon catheter, ureteral stent), self-induced foreign body
- Related to bladder augmentation and urinary diversion
- Bladder calculi is more common in male population
- Age of distribution is bimodal (peak at 3 years in pediatric age group and 60 yrs. in adult population
- Asymptomatic presentation
- Pain: at the suprapubic region; exacerbated on exercise and sudden movement; may be referred to the tip of penis, scrotum, labia majora or perineum
- Terminal hematuria
- Most common presentation of bladder calculi; due to abrasion of bladder trigone by the stone
- Lower urinary tract symptoms
- Frequency intermittency, urgency, urge incontinence
- Pediatric patients
- Pulling of the penis (pathognomonic of bladder stone), difficulty in micturition, enuresis
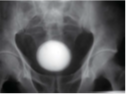
- Xray KUB: Most of the bladder stones are radiopaque
- USG KUB: First-line imaging modality in the both adults and children; low sensitivity but high specificity
- CT KUB: A useful imaging modality particularly where USG is inconclusive
- Cytoscopy: Most accurate method of detecting bladder calculi
- Medical Management: Chemo dissolution may be considered for management of encrustation over catheter tip
- Extracorporeal Shockwave Lithotripsy
- Percutaneous Cystolithotomy
- Cystolitholapaxy: Medical breakage of stone
- One of the common urologic diseases
- Commonly found in adult male patients
- Randall's plaque: Calcium plaque deposited in the interstitial tissue of renal papilla, acts
as a nidus for stone formation
- Calcium is the most common component of urinary calculi
- Events during formation of stone formation
- State of saturation
- Nucleation
- Aggregation
- Inhibitors of crystal nucleation
- Nephrocalcin
- Uropontin
- Tamm-Harsfall protein
- Inhibitors of stone formation
- Diseases associated stone formation
- Ureteropelvic junction obstruction
- Horseshoe kidney
- Ureretral stricture
- Ureterocele
- Calyceal diverticulum
- Medullary sponge kidney
- Drugs associated with stone formation
- Indinavir
- Allopurinol
- Acetazolamide
- Quinolones
- Furosemide
- Calcium oxalate stone: Most common type, small, hard and covered with irregular projections,
causing hematuria, radiopaque
- Calcium phosphate stone: Common in women, in younger age group, radiopaque
- Brushite stone: Hardest urinary stone, resistant to ESWL, high risk of recurrence,
radiopaque
- Uric acid stone: Associated with hyperuricosuria and hyperuricemia, use of salicylates,
probenecid; hard and smooth; often multiple; radiolucent
- Infection stone: Either struvite stones(magnesium ammonium phosphate) or calcium carbonate
apatite stones; associated with UTI by urea-splitting organisms; radiopaque
- Cystine stone: Multiple, very hard, risk of recurrence; poor radiopaque
- Xanthine stone: Associated with heredirary xanthinuria; radiolucent
- Fixed pain at the renal angle: Most common symptom
- Asymptomatic: Staghorn calculi
- Hematuria: Microscopic or macroscopic
- X-ray KUB: Uric acid and cystine stone not visualized
- Non-contrast helical CT: Imaging modality of choice for diagnosis of acute flank pain
- USG: Poor sensitivity but high specificity
- Urine analysis: Culture, crystalluria
- Metabolic evaluation: For specific group of patients
- Expectant management: Less than 5 mm stone, use of alpha antagonist(commonly tamsulosin), hydration- spontaneous passage of stone
- Medical management: Increased fluid intake, intake of citrus juice, DASH diet
- Extracorporeal Shockwave Lithotripsy
- Percutaneous nephrolithotomy
- Open nephrolithotomy, pyelolithotomy